










By Ward Dean, M.D.
Acarbose (Glucobay®, Precose®) is a drug approved for use in (1) insulin-dependent diabetes mellitus (Type I), (2) adult-onset diabetes mellitus (AODM, or Type II), and (3) those who suffer from “impaired glucose tolerance.” As I’ve previously pointed out, virtually everyone over the age of 35 is probably functionally glucose intolerant to some degree (Fig. 1). Using even the strictest orthodox criteria, it is estimated that up to 20% of Caucasians between the ages of 65 and 75 years have Type II Diabetes-and an additional 23% have “impaired glucose tolerance” (2).
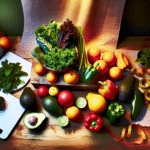
To understand how acarbose works, a review of a few basics of carbohydrate metabolism is in order. Starches and complex sugars are broken down in the digestive tract into simple sugars, which are then absorbed by the body (in the lower small intestine and colon). These simple sugars are used for energy, or stored (as glycogen or fat).
Enzymes are essential to break down the complex carbohydrates into sugars. Certain groups of enzymes are critical to the final steps in the digestion of carbohydrates. One of these groups is the alpha-glucosidases. Alpha glucosidases enhance the breakdown of maltose, isomaltose, glucoamylose and sucrose (table sugar). Acarbose acts as a potent competitive inhibitor of intestinal brush border alpha glucosidases that are essential for the breakdown of starches, dextrins, maltose, and sucrose to absorbable monosaccharides (Fig. 2). Because of its specificity for alpha glucosidases, beta glucosidases such as lactases are not affected by acarbose. Glucose is also not affected by acarbose. Consequently, glucose and lactose are absorbed normally when acarbose is taken.
Effects of Acarbose
Acarbose delays carbohydrate digestion and absorption (Fig. 3). Consequently, it delays and flattens post-meal rises in glucose and insulin (5, 6) (Fig. 4). Fasting and post-meal triglyceride levels are decreased (7,8) (probably due to the reduced insulin response) (3), and reductions in low-density lipoproteins (LDL) and increases in high-density lipoproteins (HDL) have been reported (9).
Glycosylated haemoglobin (hemoglobin A1c [HbA1c]) is a screening and diagnostic test for diabetes, as well as a biomarker of aging (indicator of biological age). HbA1c tends to increase progressively with age in non-diabetic subjects (Fig. 5) (10). Acarbose has been demonstrated in numerous studies to significantly reduce HbA1c (3, 11, 12) (Fig. 6). The reduction in HbA1c has a number of other beneficial effects, including decreased glycation of glomerular basement membranes, decreased advanced glycosylation end product (AGE) formation in connective tissue, decreased cataract formation, and prevention of neuropathy and retinopathy (13).
In addition, of particular significance with respect to the mechanism of aging proposed by Dilman’s neuroendocrine theory of aging, Balfour and McTavish (14) speculated that Acarbose might improve insulin sensitivity (as indicated by decreasing fasting blood glucose). Chiasson, et al (5) also believed Acarbose improved insulin sensitivity, based on their finding that patients taking acarbose experienced an upward trend in post-meal C-peptide levels. Furthermore, acarbose appears to prevent or delay the progressive deterioration in pancreatic beta cells that routinely occurs in patients with Type 2 DM (2).
Other benefits of alpha glucosidase inhibitors are their ability to prevent or attenuate diabetic nephropathic lesions (15), and one study even reported an improvement in cognitive function in both animals and elderly patients given Acarbose (16). Because acarbose does not result in hypoglycemia, it can be safely used by those who suffer from reactive hypoglycemia—and will probably benefit the condition due to its insulin-modulating properties.
In 2003, results from the STOP-NIDDM trial were reported (17). The trial was an international, multicentre double blind trial involving patients from Canada, Germany, Austria, Norway, Denmark, Sweden, Finland, Israel and Spain, from 1998-2001, involving nearly 1,500 patients with impaired glucose tolerance (IGT). The patients were randomized to receive placebo or 100 mg Acarbose, three times daily. The scientists wanted to evaluate whether Acarbose could prevent coronary artery disease, hypertension, congestive heart failure, or peripheral vascular disease.

The results of the study were dramatic. During the slightly more than three years of the study, 19 subjects taking placebo suffered heart attacks, compared to only 2 in the group taking Acarbose (Fig. 7). Acarbose treatment also had a significant effect on the risk of developing hypertension. Of 682 patients in the Acarbose group, only 78 developed hypertension (11%) vs 115 (17%) of those (682) in the placebo group (Fig. 8). The authors added that Acarbose treatment was associated with a significant reduction in body weight, BMI (Body Mass Index), waist circumference, blood pressure, 2-hour glucose concentrations, and triglyceride levels. They concluded that Acarbose treatment was associated with a significant reduction in the incidence of cardiovascular disease and hypertension.
In 2011, scientists presented a comprehensive schematic to connect the plethora of benefits that have been attributed to this remarkable medication (Fig. 9)
Acarbose for Weight Loss
Animal studies with acarbose have consistently shown that Acarbose has a body fat-lowering action. Balfour and McTavish (14) reported that Acarbose caused a dose-dependent reduction in body weight gain of genetically obese and hyperinsulinemic rats. In higher doses, acarbose even caused a dramatic loss in weight (Fig 10).
Many studies have reported a beneficial effect of alpha glucosidase inhibitors on bodyweight in humans (9, 11, 20-22), although the effect was usually reported as “moderate.” Acarbose also demonstrated the ability to retard “relapse weight gain” in overweight patients who had lost weight before beginning treatment with Acarbose (23, 24).
In view of the salutary effect that Acarbose has on blood sugar, insulin, lipids and HbA1c, I was at first surprised at the modest weight loss reported by participants in the studies (especially compared to the significant benefit I routinely observe in my patients). However, upon reflection, the modest effects of Acarbose as a weight loss agent in the above studies can be understood. As noted, weight loss was a usual finding in the animal studies. Most animal studies were done on normal (non-diabetic) or obese animals. However, the human studies were quite different, as the overwhelming majority of subjects were diabetic (or had impaired glucose tolerance)—and were often simultaneously treated with sulfonylureas and/or insulin. Diabetics characteristically gain weight, due to insulin resistance and hyperinsulinemia. Sulfonylurea drugs or insulin are notorious for causing additional weight gain (Metformin, which usually results in loss of body fat, was not commonly used in most of the earlier studies cited above).
More recent studies, however, have shown much more positive results—since the drugs used were Acarbose alone, or Acarbose combined with Metformin. In a large-scale observational study of some 15,000 patients in China, Taiwan, the Middle-East, Morocco, Poland, Indonesia, Pakistan and the Philippines, with a follow-up of three years, a notable weight decrease was seen in all treatment groups (Acarbose alone, or Acarbose combined with Metformin and sulfonylureas or insulin) (25). In an even more recent study in China, 784 newly-diagnosed diabetics were placed on Acarbose or Metformin. After 48 weeks, the scientists determined that Acarbose had similar efficacy to Metformin (in terms of glycemic control), but that more bodyweight was lost in the Acarbose-treated group (26).
Adverse effects and safety
Acarbose is a very safe drug; only about 1-2% is absorbed systemically. The most frequent side effects are all due to the unabsorbed carbohydrates, which ferment in the colon and can cause sometimes uncomfortable or embarrassing increased gas production, abdominal cramps, bloating and even diarrhea (Fig. 11). These effects can be minimized by taking the lowest effective dose—i.e., below that which causes the gastrointestinal distress. Continued use usually results in a reduction or resolution of these symptoms. As some tolerance seems to develop, dosages can be increased to the maximum recommended dosage of 300 mg daily.
In 1988, Clissold and Edwards (6) reported that “from the large clinical studies reported to date, acarbose—even after treatment for up to 5 years-does not produce any clinically significant adverse effects on biochemical and hematological parameters” (emphasis added). In another large placebo controlled study, doses of acarbose as large as 200 mg three times daily had no toxic effect according to the results of hematologic and biochemical profiles, including liver function tests (5) (although these high doses did cause a higher incidence of abdominal side effects, as indicated in Fig. 11).
Acarbose is contraindicated in people with inflammatory bowel disease, colonic ulceration or partial intestinal obstruction, predisposition to intestinal obstruction, chronic intestinal disease associated with marked disorders of absorption or digestion, conditions which might be exacerbated by increased intestinal gas formation (like hernias), or impaired hepatic function.
Acarbose works best when it is combined with food. When taken as a tablet, it is only ¼ as effective as when consumed in powdered form (Fig. 12). O’dea and Turton (28) recommended that Acarbose be marketed as a powder rather than a tablet, so it could be mixed into the carbohydrate components of a meal.
Since Acarbose is not available as a powder, and is actually pleasant-tasting, I suggest that it be chewed with food at the beginning of meal or when consuming a starchy snack. I recommend that Acarbose be started at as little as 25 mg daily, to minimize side effects, and gradually advance the dosage and frequency as tolerance develops, up to a maximum dosage of 100 mg three times daily, chewed with meals. Of course, if one is on a strict high protein/”Atkins Diet,” Acarbose is not necessary.
Conclusion
I believe that acarbose, like metformin; will become increasingly recognized for its potential caloric-restriction-mimicking/anti-aging, cardio-protective and anti-obesity effects. In fact, Acarbose and Metformin can be taken together, potentiating each other’s beneficial effects. Curiously, despite the well-documented safety and efficacy of Acarbose, it is not well known in the west—and many pharmacies have to “special order” it for my patients. Consequently, I was surprised to learn recently that alpha glucosidase inhibitors like Acarbose are the most popularly prescribed glucose-lowering agents in China. (29).
This content was originally published here.








{kind=link}